
Home / Blog / Thoracic Surgery / Primary vs Secondary Pneumothorax
Primary vs. Secondary Pneumothorax: When Does a Collapsed Lung Need Surgery?
What Is a Pneumothorax?
A pneumothorax, commonly known as a collapsed lung, happens when air escapes from the lung and becomes trapped in the space between the lung and the chest wall. As that trapped air builds up, it presses on the lung and stops it from expanding normally with each breath.
Doctors divide the condition that occurs without an injury — called spontaneous pneumothorax — into two categories based on what caused it, and the distinction matters a great deal for how urgently surgery is considered.
Key Takeaways
- Primary pneumothorax affects young, tall, thin adults with otherwise healthy lungs.
- Secondary pneumothorax complicates an existing lung disease and is generally more serious.
- A second collapse on the same side pushes recurrence risk above 60%.
- VATS (video-assisted thoracoscopic surgery) is the modern gold-standard treatment.
The Two Main Types of Pneumothorax
| Feature | Primary (PSP) | Secondary (SSP) |
|---|---|---|
| Underlying lung disease | None | Yes — COPD, asthma, cystic fibrosis, infection |
| Typical age | 15–34 years | Older adults |
| Body type | Tall, thin | Varies |
| Usual cause | Ruptured apical bleb | Weakened, diseased lung tissue |
| Seriousness | Lower | Higher — often needs faster action |
When Is Surgery Necessary?
Many first-time, small pneumothoraces resolve with observation, oxygen therapy, or temporary chest tube drainage alone. Surgery becomes the recommended path only under specific circumstances.
Surgery for Primary Spontaneous Pneumothorax (PSP)
- Recurrence — a second collapse on the same side raises the chance of another to over 60%.
- Persistent air leak — air keeps leaking through the chest tube for more than 3–5 days.
- Bilateral pneumothorax — both lungs collapse at once; rare, but a medical emergency.
- High-risk occupations — pilots, scuba divers, or people in remote areas are often offered surgery after the first episode.
Surgery for Secondary Spontaneous Pneumothorax (SSP)
Because the underlying lung is already diseased, surgeons tend to recommend surgery much earlier — often during the first episode, provided the patient is medically fit for anesthesia, since another collapse could become life-threatening.
The Gold-Standard Treatment: VATS Surgery
Video-Assisted Thoracoscopic Surgery (VATS) is the preferred modern surgical approach. Instead of a large open-chest incision, VATS uses just 1–3 small incisions, each roughly 1–2 cm, between the ribs — resulting in less pain and a faster recovery.
What Happens During VATS?
1. Camera Inspection
A tiny camera (thoracoscope) is inserted through a small incision, letting the surgeon examine the lung surface in high definition on a monitor.
2. Removing the Weak Area (Bullectomy / Wedge Resection)
The surgeon locates the leaking bleb and removes it with a specialized surgical stapler.
3. Pleurodesis
To help prevent a future collapse, the surgeon creates adhesion between the lung and the chest wall — through mechanical abrasion or sterile medical talc — eliminating the space where air could collect again.
Inside the Operating Room
The thoracoscopy tower displays a magnified, high-definition view throughout the procedure, allowing the entire surgical team to follow every step in real time — from initial inspection through to the final check of the staple line.
Why Is VATS Preferred?
- Smaller incisions than open surgery
- Less postoperative pain
- Shorter hospital stay
- Faster recovery
- Better cosmetic results
- Lower recurrence rates
Frequently Asked Questions
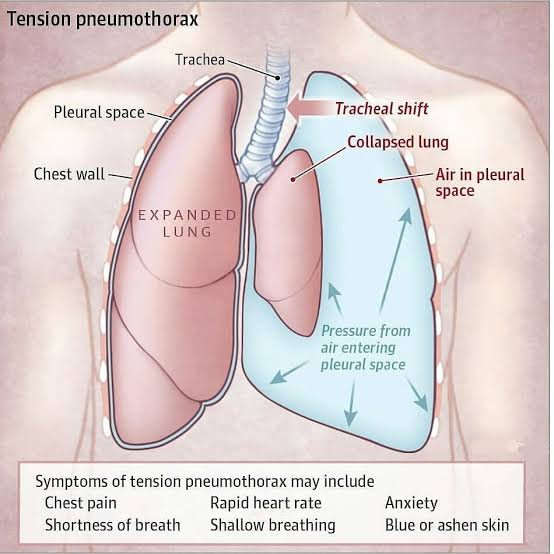
A small pneumothorax is often manageable, but a tension pneumothorax — where pressure builds rapidly — is a medical emergency requiring immediate treatment.
Most patients go home within a few days and return to light activity within 1–2 weeks, though full recovery timelines vary by case.
VATS with pleurodesis substantially lowers recurrence risk compared with chest-tube drainage alone, though no procedure eliminates the risk entirely.
No — treatment targets the affected lung. Bilateral pneumothorax, where both lungs collapse together, is rare and is treated as an emergency.
Yes — this is called a spontaneous pneumothorax, and it can be primary (no underlying disease) or secondary (linked to an existing lung condition).
Most patients tolerate VATS well, but individual suitability depends on overall lung function and fitness for anesthesia, which your surgeon will assess.
The Bottom Line
Not every collapsed lung needs an operation — but recurrence, a persistent air leak, bilateral involvement, or an underlying lung disease all shift the balance toward surgery, and toward doing it sooner rather than later. VATS has made that surgery far less invasive than it once was, with a quicker return to normal life.
Concerned About a Collapsed Lung?
If you or a family member has experienced a pneumothorax, an evaluation with a thoracic surgeon can clarify whether observation or surgery is the right next step.